
Payment and Equity for Birthworkers
Ricardo Levins Morales from an article in The Forge
It is widely understood that there is a crisis in perinatal care in the United States. (See Maternity Care in the United States: We Can - and Must - Do Better from Nat’l Partnership for Women and Families, for context).
It is not just that something isn’t working in the interactions between providers and patients (though that is part of the problem as indicated in measures like Giving Voice to Mothers study).
The structure of perinatal care is also part of the problem. For example, it is built in to the structure that most providers of perinatal care are physicians and most births in the U.S. occur in hospitals (see for example this video from Vox and ProPublica and this report from the Commonwealth Fund comparing the U.S. to ten comparable countries).
Fixing the problem requires changing the structure. One part of the structure is how the money flows. This is why it is so important whether, how, and how-much birthworkers are paid.
This is part of why the 2021 Birth Equity Bills included a requirement that both public and private insurance in Colorado reimburse providers in a manner that:
promotes high-quality, cost-effective, and evidence-based care
promotes high-value evidence-based payment models
prevents risk in subsequent pregnancies
These requirements are now law in Colorado, see C.R.S § 10-16-104 and § 25.5-4-425, and are aimed at addressing both the lack of evidence-basis for much of what happens in perinatal care, and the existence of strong data supporting integration of midwives and doulas. See, for example, Maternity Care in the United States: We Can - and Must - Do Better from Nat’l Partnership for Women and Families and Expanding the Perinatal Workforce through Medicaid Coverage of Doula and Midwifery Services, from the National Academy for State Health Policy..
Despite these laws, inequities continue and more work needs to be done to realize these goals.
These Fact Sheets are also useful for understanding what is happening in Colorado:
Elephant Circle’s Statement on the Governor’s Budget Request for Reimbursement of Doulas
Barriers to Reimbursement for CPMs and Freestanding Birth Centers in Colorado
But the problem isn’t just about the healthcare system, it is also about a system-wide failure to value, plan for, and invest in care-work (see this interview with the Culture Change Directors at Caring Across Generations and the National Domestic Workers Alliance, see also “Care Can’t Wait,” about creating a comprehensive care infrastructure).
We lack the infrastructure to support the care humans need, including in the perinatal period. Birthworkers are part of the solution because of how care is woven into the work. But if the system they work in doesn’t value care then their existence in the system won’t ensure care matters (and they may feel uncared-for as well).
We want to help transform the system to one that values care and invests in it like the infrastructure that it is.
For additional context:
Paying nonclinical birthworkers as part of the healthcare system isn’t simple since the way payments work in the system isn’t simple. To get a sense of the complexity of payment in the U.S. healthcare system, these two charts illustrate how the money flows. This is also how it flows in the perinatal care system.
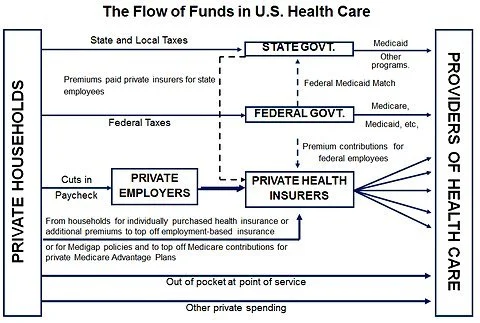
From Economix Blogs at the New York Times
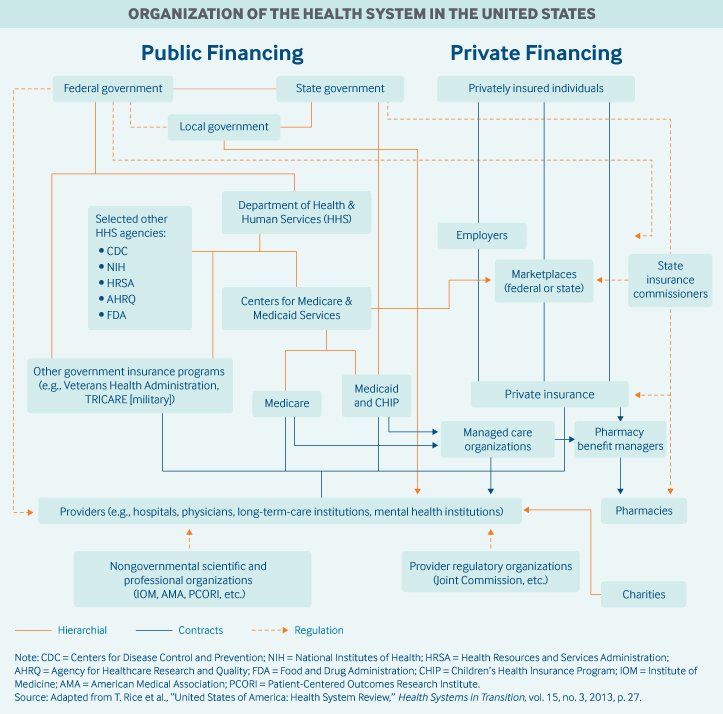
From the Commonwealth Fund
Part of the reason birthworkers, like doulas, are helpful is because this system is not good at ease, continuity, or flow for the patient - it’s organized around other interests as illustrated in these graphics - so having someone help navigate that chaos can be helpful to the patient.
Some other nonclinical providers that have been used in this way is Community Health Workers. (See this article to get a sense of how community health workers are utilized and considered in the system, and this article about sustainable financing for them). The following graphic from the article is illustrative.
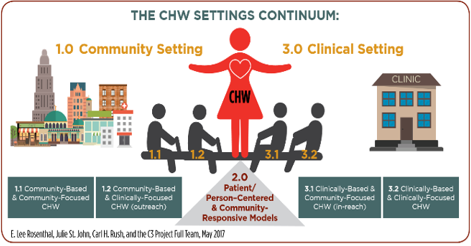
From the article linked above.